| Trabecular edema | |
|---|---|
| Other names | Bone marrow edema (BME, first used in 1988 [1]), bone marrow lesion (BML) |
 | |
| A schematic diagram showing the mechanism of bone marrow edema, adapted from.[2] | |
| Symptoms | Joint pain, effusion, warmth. |
| Types | Primary bone marrow edema, secondary bone marrow edema. |
| Causes | (For secondary BME) Trauma, degenerative lesions, inflammatory lesions, ischaemic lesions, infectious lesions, metabolic/endocrine lesions, iatrogenic lesions. |
| Risk factors | Sex, age, occupation, history of physical trauma, obesity, previous bone marrow damage, immunosuppressive/hormonal treatments, relevant medical conditions. |
| Diagnostic method | Magnetic resonance imaging (MRI). |
| Differential diagnosis | Ultrasound scans, computed tomography (CT) scans. |
| Treatment | Core decompression, pharmaceutical treatment, extracorporeal shock wave therapy (ESWT). |
| Medication | Non-steroidal anti-inflammatory drugs (e.g. Iloprost). |
Trabecular edema, also known as bone marrow edema (BME), is a traditional term describing the interstitial fluid accumulation at the trabecular bone marrow. The term was first used in 1988,[1] referring to the changes in the bone marrow due to inflammation.[3] Bone marrow edema was later renamed to bone marrow lesion (BML), as later studies show that the increased fluid content in the trabecular bone was more likely caused by inflammatory responses (e.g. increased vascularization, lymphocyte infiltration) instead of fluid influx (i.e. edema).[2][4][5] Hence, this narrows down the condition to the damage at the articular surface of the trabecular bones.[2] Despite so, the terms BME and BML are still used interchangeably in radiology.[6]
This condition normally affects the musculoskeletal system, and commonly manifests in lower extremities, including but not limited to the feet, ankle joints, knee joints, and hip joints.[2][7] Common signs and symptoms include pain, joint swelling, and limited joint functionality.[8] BME can be further separated into two types, based on their causes: primary BME and secondary BME. Primary BME, also called spontaneous BME or bone marrow edema syndrome (BMES), means bone marrow edema without obvious causes. Secondary BME meanwhile refers to bone marrow edema caused by another condition.[9] It is usually diagnosed with magnetic resonance imaging (MRI), supplemented with ultrasound scans.[2] However, BME cannot be detected by X-ray or computerized tomography (CT) scans directly,[2][5] but they are helpful in differential diagnosis.[5][9] Minor cases are usually treated through proper resting and taking non-steroidal anti-inflammatory drugs (NSAIDs), while steroid therapy or even surgery may be needed for more serious ones.[10][11][12][13]
Pre-existing conditions like arthritis or bone cancer induce stress onto the bones, leading to a greater risk of BME within patients suffering from those conditions.[14] Other studies also list high bone density as a risk factor to some local bone marrow lesions.[15][16] Sex,[17][18] age, earlier immunosuppressive treatments,[19] or pre-existing physical trauma are all risk factors of bone marrow edema.[20][21][22][23] Prevention of bone marrow edema is difficult due to the vast variety of causes, but detecting bone marrow edema can predict subsequent progression to bone erosion[9][24] or the need to replace the joint.[9][25]
Signs and symptoms

Common symptoms of BME include joint effusion, joint pain, and warmth, which are related to joint inflammation.[2] Patients usually have severe pain in the bones or joints, which often leads to limitations in functionality that harm their quality of life.[8]
Primary bone marrow edema
In primary bone marrow edema patients, initial painful symptoms usually appear in the first month, followed by a peak in pain level two months after onset.[7] The transient increase in interstitial fluid leads to increased intraosseous pressure and aggravated neurovascular bundles.[26] The symptoms typically fade a few months after the phase with maximum pain level,[7] which may be due to the bone remodelling abilities as new bone formation and vascular reconstruction steps are observed.[27]

Secondary bone marrow edema
In secondary bone marrow edema patients, repeated traumatic stress may disrupt the trabecular marrow structure, hence there is interstitial fluid leakage or haemorrhage inside the marrow spaces. Also, heightened blood flow or a congested vascular drainage at the bone marrow may cause BME.[26] The increased fluid content leads to an increase in intraosseous pressure as well as decreased perfusion,[28] which disturbs the neurovascular bundles and result in pain and swelling. Local cytokine production mediates the inflammatory response and thus worsens the symptoms.[26]
Pathophysiology
Bone marrow edema does not have similar histological characteristics as other types of edema, such as pulmonary edema. This is because it is commonly caused by inflammation and vascularization, resulting in displacement of bone marrow, originally rich in adipocytes, by hydrophilic material. Said material may be immune cells, particularly T and B lymphocytes, and microvessels.[2]
However, the exact mechanism that causes bone marrow edema is still unknown. It is only known that the presence of bone marrow edema is usually associated with the progression of various diseases such as osteonecrosis.[29] Different pathophysiology mechanisms are established based on the cause of the bone marrow edema. For example, if the cause of bone marrow edema is rheumatoid arthritis, the edema is attributed to the penetration sites caused by the resorption of mineralized cortical bone beneath articular cartilage.[2] These penetration sites allow the entry of inflammatory infiltrates, which could possibly be lymphocytic aggregates or invaded synovial tissue that are heavily vascularized, contributing to high water content in the bone marrow compartment.[2] As in some other causes such as renal transplantation, impairment of microcirculation could result in an increase of the intraosseous pressure.[2] The increased hydrostatic pressure causes more fluid leakage out of the capillaries, and bone marrow edema is the direct result.
A common characteristic among bone marrow edema patients is the pain experienced, due to the aggravation of the neurovascular bundle by increased intraosseous pressure.[10]
Etiology
A crucial element for a physician to diagnose BME is the ability to differentiate whether the patient suffers from primary or secondary bone marrow edema, as primary bone marrow edema could indicate stage of progression to osteonecrosis.[6] Unfortunately, interdisciplinary guidelines and management algorithms regarding BME are currently underdeveloped, resulting in repetitive checking, delayed diagnosis or treatment.
Primary bone marrow edema
Primary bone marrow edema is also referred to as spontaneous bone marrow edema, or bone marrow edema syndrome (BMES). This category of BME does not have a particular cause but is self-limiting in nature, meaning that symptoms usually resolve by themselves within three to nine months after onset without pathological consequences.[9]
There are theories proposing possible etiologies like vascular anomalies or thromboembolism, but they are yet to be proven.[10]
Secondary bone marrow edema
Secondary bone marrow edema is caused by pre-existing conditions, which may be interdisciplinary. Hence, this category of BME is commonly found in MRIs, in which the original intention was not to diagnose this particular condition. The different causes of secondary bone marrow edema are listed as follows:[2]
Trauma
Trauma events cause frequent microfractures. For instance, in transient regional osteoporosis and bone bruises, bone marrow lesions start in one skeletal region and spontaneously appear in another skeletal region with time.[30] The cause is associated with active osteoporotic changes and low bone mineral density, which allows microfractures to occur in the affected region.[31]

Degenerative lesions
Tendinitis has a strong association with bone marrow edema. A study reported around one-third of tendinitis patients have bone marrow edema, and even all cases are revealed to be an uptake in isotope scans.[32]
Osteoarthritis is another disease that has a strong association with bone marrow edema due to mechanical loading, as well as stress on the subchondral region.[33][34]
Inflammatory lesions
There exist three types of inflammatory lesions: seropositive inflammatory arthropathy, seronegative arthritis, and enthesitis. Bone marrow lesions tend to be present in inflammatory arthropathy due to increased vascularisation,[2] and are often present in sites of arthritis and enthesitis as well.[35]
Ischaemic lesions
Avascular necrosis of bone is directly related to bone marrow lesions; the severity of bone marrow lesions is correlated with the intensity of avascular osteonecrosis.[29]
Infectious lesions
Bacterial infections and bone marrow lesion development are closely related, as infection directly leads to inflammation.[36] For example, infections of the foot in diabetic patients that spread to the bone are associated with bone marrow lesions.[37]
Metabolic/Endocrine lesions
Hormonal imbalances such as severe hyperthyroidism and hyperparathyroidism, which lead to impairment of bone metabolism, could cause bone marrow edema.[23] Changes in connective tissue deposition such as uric acid composition in gout could cause bone marrow edema.[38]
Iatrogenic lesions
Damage could be done to bone marrow during surgery or radiotherapy, leading to inflammation and hence bone marrow edema as in other lesions. Patients who have undergone hormone therapy are also susceptible to bone marrow edema due to insufficient bone metabolism and high bone turnover.[19]
Osteonecrosis risk may also be increased by common immunosuppressants like cyclosporine and tacrolimus, due to the induced vasoconstriction. Drugs such as sirolimus may potentiate this effect by similar action or influencing the lipid profile.[22]
Risk factors
Bone marrow edema is usually caused by or associated with pre-existing conditions. Numerous epidemiological studies in patients with bone marrow edema have found certain patterns of characteristics among the participants; for example, certain medical conditions such as osteoporosis are substantial risk factors for developing bone marrow edema.[39] Several common risk factors are listed as follows:
- Sex; women in particular have a higher rate of contracting bone marrow edema[17]
- Age; being at least 50 years old is also a major risk factor[20]
- Occupation/Poor posture[40]
- History of physical trauma[21]
- Overweightness/Obesity[41]
- Previous damage to bone marrow due to surgery or radiation therapy[22]
- Immunosuppressive or hormonal treatments[22][23]
- Relevant medical conditions[14]
- Arthritis
- Bone cancer
- Bone infection
- Osteoporosis
- Post-renal transplantation syndrome[2]
Diagnosis
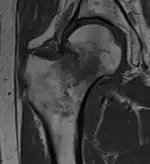
Magnetic resonance imaging (MRI)
Diagnosis of trabecular edema is primarily done via magnetic resonance imaging (MRI). The presence of edema within the bone marrow yields a visible signal on the MRI, due to displacement of the normally fatty tissue within the marrow by interstitial fluid with higher water content; this change in composition is then reflected by the MRI due to differences in the T1-weighted and T2-weighted images.[5][1]
A healthy bone is rich in fat and has lower water content, therefore it appears as bright signals on T1-weighted images and dark on T2-weighted images.[2] Conversely, regions with trabecular edema has lower fat and higher water content. Hence, they have a comparatively lower intensity than normal bone tissues on a T1-weighted image, and a higher intensity on a T2-weighted image.[42]
Ultrasound Scan
Being less sensitive compared to MRI scans, ultrasound scans are able to detect some abnormalities like joint effusion and capsular thickening, which are common in BME patients.[43]
Computed Tomography (CT) Scan
Computed tomography (CT) scans cannot directly diagnose bone marrow edema, but it is sometimes used to supplement MRI scans for differential diagnosis. It is due to its ability to show any lesions or fractures in trabecular, subchondral or chondral structures, which aids physicians to understand if there are any underlying bone pathologies leading to the observed symptoms.[9]
Treatment
Core decompression
As edema is by definition accumulation of excess fluid within body tissue, one method of treating edema is draining said excess fluid. Core decompression, otherwise often used to treat avascular necrosis, is a surgical procedure that involves drilling a hole into dead bone tissue, leading to the reduction of pressure within the bone and increase of blood flow; thus, the excess fluid can be drained and the edema treated.[13] A combination of core decompression with injection of hydroxyapatite cement into the tissue affected with bone marrow edema has been reported to significantly reduce pain levels.[44]
Pharmaceutical treatment

Another goal of treating trabecular edema is to manage the symptoms, such as pain. Nonsteroidal anti-inflammatory drugs such as Iloprost, a medication that dilates arterial vascular beds, have been proven to aid in treating bone marrow lesions when administered in an intravenous manner, resulting in reduction of pain and restoration of functionality in affected areas.[10][11][12]

Physical treatment
Yet another method of treating bone marrow edema is extracorporeal shock wave therapy (ESWT), a process involving re-injury of cells via acoustic shock waves to promote regeneration of blood vessels and bone. The treatment has been proven to halve the size of areas affected by edema after six months of administration.[45]
Research
Recent evidence found associations between vitamin status and bone marrow edema syndrome. A pathophysiological association is found between vitamin D status, which denotes osteopenia, and bone marrow edema syndrome. The association has yet to be found to be causative. As for vitamin C, vitamin deficiency in scurvy patients is a causative factor but no current literature reports acute and subacute vitamin C deficiency. For future research, more advanced study designs such as randomized clinical trials are needed to evaluate therapy by means of vitamin supplements.[46]
On the other hand, another recent literature review was performed on studies published from 2011 to 2021, investigating the efficacy of various conservative treatments of BMES. Although comparison of the studies in a highly reliable manner was difficult due to lack of standardisation of treatment methods, studies still found prospective results in treating bone marrow edema efficiently. Future studies should establish a standardised radiological score system to evaluate the areas of bone marrow edema.[47]
References
- 1 2 3 Wilson AJ, Murphy WA, Hardy DC, Totty WG (June 1988). "Transient osteoporosis: transient bone marrow edema?". Radiology. 167 (3): 757–760. doi:10.1148/radiology.167.3.3363136. PMID 3363136.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Schett G (February 2009). "Bone marrow edema". Annals of the New York Academy of Sciences. 1154 (1): 35–40. Bibcode:2009NYASA1154...35S. doi:10.1111/j.1749-6632.2009.04383.x. PMID 19250229. S2CID 9190990.
- ↑ Eriksen EF (2015-11-25). "Treatment of bone marrow lesions (bone marrow edema)". BoneKEy Reports. 4: 755. doi:10.1038/bonekey.2015.124. PMC 4662576. PMID 26644910.
- ↑ Thiryayi WA, Thiryayi SA, Freemont AJ (July 2008). "Histopathological perspective on bone marrow oedema, reactive bone change and haemorrhage". European Journal of Radiology. 67 (1): 62–67. doi:10.1016/j.ejrad.2008.01.056. PMID 18337044.
- 1 2 3 4 Manara M, Varenna M (July 2014). "A clinical overview of bone marrow edema". Reumatismo. 66 (2): 184–196. doi:10.4081/reumatismo.2014.790. PMID 25069499.
- 1 2 Patel S (May 2014). "Primary bone marrow oedema syndromes". Rheumatology. 53 (5): 785–792. doi:10.1093/rheumatology/ket324. PMID 24080251.
- 1 2 3 Mirghasemi SA, Trepman E, Sadeghi MS, Rahimi N, Rashidinia S (December 2016). "Bone Marrow Edema Syndrome in the Foot and Ankle". Foot & Ankle International. 37 (12): 1364–1373. doi:10.1177/1071100716664783. PMID 27587374. S2CID 22940741.
- 1 2 Marcacci M, Andriolo L, Kon E, Shabshin N, Filardo G (May 2016). "Aetiology and pathogenesis of bone marrow lesions and osteonecrosis of the knee". EFORT Open Reviews. 1 (5): 219–224. doi:10.1302/2058-5241.1.000044. PMC 5367544. PMID 28461951.
- 1 2 3 4 5 6 Baumbach SF, Pfahler V, Bechtold-Dalla Pozza S, Feist-Pagenstert I, Fürmetz J, Baur-Melnyk A, et al. (February 2020). "How We Manage Bone Marrow Edema-An Interdisciplinary Approach". Journal of Clinical Medicine. 9 (2): 551. doi:10.3390/jcm9020551. PMC 7074543. PMID 32085459.
- 1 2 3 4 Davis DD, Kane SM (2023). "Bone Marrow Edema Syndrome". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 32644602. Retrieved 2023-03-26.
- 1 2 Röhner E, Zippelius T, Steindl D, Fussi J, Perka C (December 2014). "Effects of intravenous iloprost therapy in patients with bone marrow oedema of the foot and ankle". European Journal of Orthopaedic Surgery & Traumatology. 24 (8): 1609–1616. doi:10.1007/s00590-013-1320-0. PMID 24048706. S2CID 5844570.
- 1 2 Meizer R, Radda C, Stolz G, Kotsaris S, Petje G, Krasny C, et al. (April 2005). "MRI-controlled analysis of 104 patients with painful bone marrow edema in different joint localizations treated with the prostacyclin analogue iloprost". Wiener Klinische Wochenschrift. 117 (7–8): 278–286. doi:10.1007/s00508-005-0326-y. PMID 15926619. S2CID 6466752.
- 1 2 Zippelius T, Strube P, Matziolis G, Röhner E, Böhle S, Brodt S (November 2020). "Cone beam-navigated core decompression of bone marrow edema syndrome". Archives of Orthopaedic and Trauma Surgery. 140 (11): 1603–1609. doi:10.1007/s00402-020-03339-0. PMID 31960167. S2CID 210717263.
- 1 2 Coates PT, Tie M, Russ GR, Mathew TH (May 2002). "Transient bone marrow edema in renal transplantation: a distinct post-transplantation syndrome with a characteristic MRI appearance". American Journal of Transplantation. 2 (5): 467–470. doi:10.1034/j.1600-6143.2002.20512.x. PMID 12123214. S2CID 23855997.
- ↑ Lo GH, Hunter DJ, Zhang Y, McLennan CE, Lavalley MP, Kiel DP, et al. (September 2005). "Bone marrow lesions in the knee are associated with increased local bone density". Arthritis and Rheumatism. 52 (9): 2814–2821. doi:10.1002/art.21290. PMID 16145676.
- ↑ Crema MD, Roemer FW, Marra MD, Guermazi A (August 2009). "Magnetic resonance imaging assessment of subchondral bone and soft tissues in knee osteoarthritis". Rheumatic Disease Clinics of North America. 35 (3): 557–577. doi:10.1016/j.rdc.2009.08.003. PMID 19931803.
- 1 2 "Osteoarthritis Risk Factors in Women & How to Prevent Them". Hospital for Special Surgery. Retrieved 2023-04-12.
- ↑ Braun J, Baraliakos X, Bülow R, Schmidt CO, Richter A (January 2022). "Striking sex differences in magnetic resonance imaging findings in the sacroiliac joints in the population". Arthritis Research & Therapy. 24 (1): 29. doi:10.1186/s13075-021-02712-7. PMC 8772059. PMID 35057838.
- 1 2 Oehler N, Mussawy H, Schmidt T, Rolvien T, Barvencik F (December 2018). "Identification of vitamin D and other bone metabolism parameters as risk factors for primary bone marrow oedema syndrome". BMC Musculoskeletal Disorders. 19 (1): 451. doi:10.1186/s12891-018-2379-x. PMC 6303903. PMID 30579337.
- 1 2 Shimodaira H, Hatakeyama A, Suzuki H, Takada S, Murata Y, Sakai A, Uchida S (December 2021). "The prevalence and risk factors of pubic bone marrow edema in femoroacetabular impingement and hip dysplasia". Journal of Hip Preservation Surgery. 8 (4): 318–324. doi:10.1093/jhps/hnab081. PMC 9052425. PMID 35505801.
- 1 2 Tarantino U, Greggi C, Cariati I, Manenti G, Primavera M, Ferrante P, et al. (October 2021). "Reviewing Bone Marrow Edema in Athletes: A Difficult Diagnostic and Clinical Approach". Medicina. 57 (11): 1143. doi:10.3390/medicina57111143. PMC 8625152. PMID 34833361.
- 1 2 3 4 Elder GJ (December 2006). "From marrow oedema to osteonecrosis: common paths in the development of post-transplant bone pain". Nephrology. 11 (6): 560–567. doi:10.1111/j.1440-1797.2006.00708.x. PMID 17199798. S2CID 23210159.
- 1 2 3 Mepani JB, Findling JW (April 2009). "Reversible bone marrow edema of the hip due to severe hypothyroidism". The Journal of Clinical Endocrinology and Metabolism. 94 (4): 1068. doi:10.1210/jc.2008-1523. PMID 19349470. S2CID 45839201.
- ↑ Haavardsholm EA, Bøyesen P, Østergaard M, Schildvold A, Kvien TK (June 2008). "Magnetic resonance imaging findings in 84 patients with early rheumatoid arthritis: bone marrow oedema predicts erosive progression". Annals of the Rheumatic Diseases. 67 (6): 794–800. doi:10.1136/ard.2007.071977. PMID 17981915. S2CID 26085720.
- ↑ Tanamas SK, Wluka AE, Pelletier JP, Pelletier JM, Abram F, Berry PA, et al. (December 2010). "Bone marrow lesions in people with knee osteoarthritis predict progression of disease and joint replacement: a longitudinal study". Rheumatology. 49 (12): 2413–2419. doi:10.1093/rheumatology/keq286. PMID 20823092.
- 1 2 3 Eustace S, Keogh C, Blake M, Ward RJ, Oder PD, Dimasi M (January 2001). "MR imaging of bone oedema: mechanisms and interpretation". Clinical Radiology. 56 (1): 4–12. doi:10.1053/crad.2000.0585. PMID 11162690.
- ↑ Plenk H, Hofmann S, Eschberger J, Gstettner M, Kramer J, Schneider W, Engel A (January 1997). "Histomorphology and bone morphometry of the bone marrow edema syndrome of the hip". Clinical Orthopaedics and Related Research (334): 73–84. PMID 9005898.
- ↑ Aaron RK, Dyke JP, Ciombor DM, Ballon D, Lee J, Jung E, Tung GA (November 2007). "Perfusion abnormalities in subchondral bone associated with marrow edema, osteoarthritis, and avascular necrosis". Annals of the New York Academy of Sciences. 1117 (1): 124–137. Bibcode:2007NYASA1117..124A. doi:10.1196/annals.1402.069. PMID 18056039. S2CID 22873619.
- 1 2 Ito H, Matsuno T, Minami A (June 2006). "Relationship between bone marrow edema and development of symptoms in patients with osteonecrosis of the femoral head". AJR. American Journal of Roentgenology. 186 (6): 1761–1770. doi:10.2214/AJR.05.0086. PMID 16714671.
- ↑ Emad Y, Ragab Y, El-Shaarawy N, Rasker JJ (November 2012). "Transient osteoporosis of the hip, complete resolution after treatment with alendronate as observed by MRI description of eight cases and review of the literature" (PDF). Clinical Rheumatology. 31 (11): 1641–1647. doi:10.1007/s10067-012-2060-y. PMID 22933125. S2CID 19584180.
- ↑ Guardiano SA, Katz J, Schwartz AM, Brindle K, Curiel R (October 2004). "Fracture complicating the bone marrow edema syndrome". Journal of Clinical Rheumatology. 10 (5): 269–274. doi:10.1097/01.rhu.0000141509.18395.3c. PMID 17043527. S2CID 29999514.
- ↑ Flemming DJ, Murphey MD, Shekitka KM, Temple HT, Jelinek JJ, Kransdorf MJ (October 2003). "Osseous involvement in calcific tendinitis: a retrospective review of 50 cases". AJR. American Journal of Roentgenology. 181 (4): 965–972. doi:10.2214/ajr.181.4.1810965. PMID 14500211.
- ↑ Bennell KL, Creaby MW, Wrigley TV, Bowles KA, Hinman RS, Cicuttini F, Hunter DJ (June 2010). "Bone marrow lesions are related to dynamic knee loading in medial knee osteoarthritis". Annals of the Rheumatic Diseases. 69 (6): 1151–1154. doi:10.1136/ard.2009.118182. PMID 19910299. S2CID 10401516.
- ↑ Felson DT, McLaughlin S, Goggins J, LaValley MP, Gale ME, Totterman S, et al. (September 2003). "Bone marrow edema and its relation to progression of knee osteoarthritis". Annals of Internal Medicine. 139 (5 Pt 1): 330–336. doi:10.7326/0003-4819-139-5_part_1-200309020-00008. PMID 12965941. S2CID 23291712.
- ↑ Erdem CZ, Tekin NS, Sarikaya S, Erdem LO, Gulec S (September 2008). "MR imaging features of foot involvement in patients with psoriasis". European Journal of Radiology. 67 (3): 521–525. doi:10.1016/j.ejrad.2007.08.005. PMID 17997068.
- ↑ Jäger M, Tillmann FP, Thornhill TS, Mahmoudi M, Blondin D, Hetzel GR, et al. (2008). "Rationale for prostaglandin I2 in bone marrow oedema--from theory to application". Arthritis Research & Therapy. 10 (5): R120. doi:10.1186/ar2526. PMC 2592809. PMID 18834533.
- ↑ Peters EJ, Lipsky BA (September 2013). "Diagnosis and management of infection in the diabetic foot". The Medical Clinics of North America. 97 (5): 911–946. doi:10.1016/j.mcna.2013.04.005. PMID 23992901.
- ↑ Carter JD, Kedar RP, Anderson SR, Osorio AH, Albritton NL, Gnanashanmugam S, et al. (November 2009). "An analysis of MRI and ultrasound imaging in patients with gout who have normal plain radiographs". Rheumatology. 48 (11): 1442–1446. doi:10.1093/rheumatology/kep278. PMID 19745028.
- ↑ Kotwal A, Hurtado MD, Sfeir JG, Wermers RA (July 2019). "Transient Osteoporosis: Clinical Spectrum in Adults and Associated Risk Factors". Endocrine Practice. 25 (7): 648–656. doi:10.4158/EP-2018-0626. PMID 30865521. S2CID 76664615.
- ↑ Seok H, Choi SJ, Yoon JH, Song GG, Won JU, Kim JH, et al. (2017-01-18). "The Association between Osteoarthritis and Occupational Clusters in the Korean Population: A Nationwide Study". PLOS ONE. 12 (1): e0170229. Bibcode:2017PLoSO..1270229S. doi:10.1371/journal.pone.0170229. PMC 5242527. PMID 28099527.
- ↑ Lim YZ, Wang Y, Wluka AE, Davies-Tuck ML, Hanna F, Urquhart DM, Cicuttini FM (April 2014). "Association of obesity and systemic factors with bone marrow lesions at the knee: a systematic review". Seminars in Arthritis and Rheumatism. 43 (5): 600–612. doi:10.1016/j.semarthrit.2013.10.006. PMID 24287353.
- ↑ Bonadio MB, Filho AG, Helito CP, Stump XM, Demange MK (2017-01-01). "Bone Marrow Lesion: Image, Clinical Presentation, and Treatment". Magnetic Resonance Insights. 10: 1178623X17703382. doi:10.1177/1178623X17703382. PMC 5428162. PMID 28579795.
- ↑ Wang MY, Wang XB, Sun XH, Liu FL, Huang SC (November 2016). "Diagnostic value of high-frequency ultrasound and magnetic resonance imaging in early rheumatoid arthritis". Experimental and Therapeutic Medicine. 12 (5): 3035–3040. doi:10.3892/etm.2016.3695. PMC 5103740. PMID 27882112.
- ↑ Yang P, Bian C, Huang X, Shi A, Wang C, Wang K (January 2014). "Core decompression in combination with nano-hydroxyapatite/polyamide 66 rod for the treatment of osteonecrosis of the femoral head". Archives of Orthopaedic and Trauma Surgery. 134 (1): 103–112. doi:10.1007/s00402-013-1885-4. PMID 24248422. S2CID 20158344.
- ↑ d'Agostino C, Romeo P, Lavanga V, Pisani S, Sansone V (November 2014). "Effectiveness of extracorporeal shock wave therapy in bone marrow edema syndrome of the hip". Rheumatology International. 34 (11): 1513–1518. doi:10.1007/s00296-014-2991-5. hdl:2434/236603. PMID 24658812. S2CID 20340469.
- ↑ Eidmann A, Eisert M, Rudert M, Stratos I (November 2022). "Influence of Vitamin D and C on Bone Marrow Edema Syndrome-A Scoping Review of the Literature". Journal of Clinical Medicine. 11 (22): 6820. doi:10.3390/jcm11226820. PMC 9696648. PMID 36431295.
- ↑ Evola FR, Compagnoni R, Pieroni A, Tassi A, Menon A, Randelli P (2022-10-01). "The Efficacy of Conservative Treatment of Bone Marrow Edema Syndrome: A Scoping Review of the Last Ten Years of Literature". Journal of Clinical Densitometry. 25 (4): 506–517. doi:10.1016/j.jocd.2022.06.003. PMID 35987803. S2CID 251357388.