| Gestational diabetes | |
|---|---|
| Other names | Gestational diabetes mellitus (GDM) |
 | |
| Universal blue circle symbol for diabetes[1] | |
| Specialty | Obstetrics and endocrinology |
| Symptoms | Typically few symptoms[2] |
| Complications | Pre-eclampsia, stillbirth, depression, increased risk of requiring a Caesarean section[2] |
| Usual onset | Most common last three months of pregnancy[2] |
| Causes | Not enough insulin in the setting of insulin resistance[2] |
| Risk factors | Overweight, previously having gestational diabetes, family history of type 2 diabetes, polycystic ovarian syndrome[2] |
| Diagnostic method | Screening blood tests[2] |
| Prevention | Maintaining a healthy weight and exercising before pregnancy[2] |
| Treatment | Diabetic diet, exercise, insulin injections[2] |
| Frequency | ~6% of pregnancies[3] |
Gestational diabetes is a condition in which a woman without diabetes develops high blood sugar levels during pregnancy.[2] Gestational diabetes generally results in few symptoms;[2] however, it increases the risk of pre-eclampsia, depression, and of needing a Caesarean section.[2] Babies born to mothers with poorly treated gestational diabetes are at increased risk of macrosomia, of having hypoglycemia after birth, and of jaundice.[2] If untreated, diabetes can also result in stillbirth.[2] Long term, children are at higher risk of being overweight and of developing type 2 diabetes.[2]
Gestational diabetes can occur during pregnancy because of insulin resistance or reduced production of insulin.[2] Risk factors include being overweight, previously having gestational diabetes, a family history of type 2 diabetes, and having polycystic ovarian syndrome.[2] Diagnosis is by blood tests.[2] For those at normal risk, screening is recommended between 24 and 28 weeks' gestation.[2][3] For those at high risk, testing may occur at the first prenatal visit.[2]
Maintenance of healthy weight and exercising before pregnancy assist in prevention.[2] Gestational diabetes is treated with a diabetic diet, exercise, medication (such as metformin), and sometimes insulin injections.[2] Most women manage blood sugar with diet and exercise.[3] Blood sugar testing among those who are affected is often recommended four times a day.[3] Breastfeeding is recommended as soon as possible after birth.[2]
Gestational diabetes affects 3–9% of pregnancies, depending on the population studied.[3] It is especially common during the third trimester.[2] It affects 1% of those under the age of 20 and 13% of those over the age of 44.[3] A number of ethnic groups including Asians, American Indians, Indigenous Australians, and Pacific Islanders are at higher risk.[3][2] However, the variations in prevalence are also due to different screening strategies and diagnostic criteria being used. In 90% of cases, gestational diabetes resolves after the baby is born.[2] Women, however, are at an increased risk of developing type 2 diabetes.[3]
Classification
Gestational diabetes is formally defined as "any degree of glucose intolerance with onset or first recognition during pregnancy".[4] This definition acknowledges the possibility that a woman may have previously undiagnosed diabetes mellitus, or may have developed diabetes coincidentally with pregnancy. Whether symptoms subside after pregnancy is also irrelevant to the diagnosis.[5] A woman is diagnosed with gestational diabetes when glucose intolerance continues beyond 24 to 28 weeks of gestation.
The White classification, named after Priscilla White,[6] who pioneered research on the effect of diabetes types on perinatal outcome, is widely used to assess maternal and fetal risk.[7] It distinguishes between gestational diabetes (type A) and pregestational diabetes (diabetes that existed prior to pregnancy). These two groups are further subdivided according to their associated risks and management.[8]
The two subtypes of gestational diabetes under this classification system are:
- Type A1: abnormal oral glucose tolerance test (OGTT), but normal blood glucose levels during fasting and two hours after meals; diet modification is sufficient to control glucose levels
- Type A2: abnormal OGTT compounded by abnormal glucose levels during fasting and/or after meals; additional therapy with insulin or other medications is required
Diabetes which existed prior to pregnancy is also split up into several subtypes under this system:
- Type B: onset at age 20 or older and duration of less than 10 years.
- Type C: onset at age 10–19 or duration of 10–19 years.
- Type D: onset before age 10 or duration greater than 20 years.
- Type E: overt diabetes mellitus with calcified pelvic vessels.
- Type F: diabetic nephropathy.
- Type R: proliferative retinopathy.
- Type RF: retinopathy and nephropathy.
- Type H: ischemic heart disease.
- Type T: prior kidney transplant.
An early age of onset or long-standing disease comes with greater risks, hence the first three subtypes.
Two other sets of criteria are available for diagnosis of gestational diabetes, both based on blood-sugar levels.[9]
Criteria for diagnosis of gestational diabetes, using the 100 gram Glucose Tolerance Test, according to Carpenter and Coustan:[10]
- Fasting 95 mg/dl
- 1 hour 180 mg/dl
- 2 hours 155 mg/dl
- 3 hours 140 mg/dl
Criteria for diagnosis of gestational diabetes according to National Diabetes Data Group:[9][11]
- Fasting 105 mg/dl
- 1 hour 190 mg/dl
- 2 hours 165 mg/dl
- 3 hours 145 mg/dl
Risk factors
Classical risk factors for developing gestational diabetes are:[12]
- Polycystic ovary syndrome[13]
- A previous diagnosis of gestational diabetes or prediabetes, impaired glucose tolerance, or impaired fasting glycaemia
- A family history revealing a first-degree relative with type 2 diabetes
- Maternal age – a woman's risk factor increases as she gets older (especially for women over 35 years of age).
- Paternal age – one study found that a father's age over 55 years was associated with GD[14]
- Ethnicity (those with higher risk factors include African-Americans, Afro-Caribbeans, Native Americans, Hispanics, Pacific Islanders, and people originating from South Asia)
- Being overweight, obese or severely obese increases the risk by a factor 2.1, 3.6 and 8.6, respectively.[15]
- A previous pregnancy which resulted in a child with a macrosomia (high birth weight: >90th centile or >4000 g (8 lbs 12.8 oz))
- Previous poor obstetric history
- Other genetic risk factors: There are at least 10 genes where certain polymorphism are associated with an increased risk of gestational diabetes, most notably TCF7L2.[16] The MTNR1B gene is a common gene that is associated with how the body handles insulin and glucose. When this gene is not working properly, it can lead to less insulin production and higher blood glucose levels.[17]
In addition to this, statistics show a double risk of GDM in smokers.[18] Some studies have looked at more controversial potential risk factors, such as short stature.[19]
About 40–60% of women with GDM have no demonstrable risk factor; for this reason many advocate to screen all women.[20] Typically, women with GDM exhibit no symptoms (another reason for universal screening), but some women may demonstrate increased thirst, increased urination, fatigue, nausea and vomiting, bladder infection, yeast infections and blurred vision.[21]
Pathophysiology

The precise mechanisms underlying gestational diabetes remain unknown. The hallmark of GDM is increased insulin resistance. Pregnancy hormones and other factors are thought to interfere with the action of insulin as it binds to the insulin receptor. The interference probably occurs at the level of the cell signaling pathway beyond the insulin receptor.[22] Since insulin promotes the entry of glucose into most cells, insulin resistance prevents glucose from entering the cells properly. As a result, glucose remains in the bloodstream, where glucose levels rise. More insulin is needed to overcome this resistance; about 1.5–2.5 times more insulin is produced than in a normal pregnancy.[22]
Insulin resistance is a normal phenomenon emerging in the second trimester of pregnancy, which in cases of GDM progresses thereafter to levels seen in a non-pregnant woman with type 2 diabetes. It is thought to secure glucose supply to the growing fetus. Women with GDM have an insulin resistance that they cannot compensate for with increased production in the β-cells of the pancreas. Placental hormones, and, to a lesser extent, increased fat deposits during pregnancy, seem to mediate insulin resistance during pregnancy. Cortisol and progesterone are the main culprits, but human placental lactogen, prolactin and estradiol contribute, too. Multivariate stepwise regression analysis reveals that, in combination with other placental hormones, leptin, tumor necrosis factor alpha, and resistin are involved in the decrease in insulin sensitivity occurring during pregnancy, with tumor necrosis factor alpha named as the strongest independent predictor of insulin sensitivity in pregnancy.[23] An inverse correlation with the changes in insulin sensitivity from the time before conception through late gestation accounts for about half of the variance in the decrease in insulin sensitivity during gestation: in other words, low levels or alteration of TNF alpha factors corresponds with a greater chance of, or predisposition to, insulin resistance or sensitivity.[24]
It is unclear why some women are unable to balance insulin needs and develop GDM; however, a number of explanations have been given, similar to those in type 2 diabetes: autoimmunity, single gene mutations, obesity, along with other mechanisms.[25]
Though the clinical presentation of gestational diabetes is well characterized, the biochemical mechanism behind the disease is not well known. One proposed biochemical mechanism involves insulin-producing β-cell adaptation controlled by the HGF/c-MET signaling pathway. β-cell adaption refers to the change that pancreatic islet cells undergo during pregnancy in response to maternal hormones in order to compensate for the increased physiological needs of mother and baby. These changes in the β-cells cause increased insulin secretion as a result of increased β-cell proliferation.[26] HGF/c-MET has also been implicated in β-cell regeneration, which suggests that HGF/c-MET may help increase β-cell mass in order to compensate for insulin needs during pregnancy. Recent studies support that loss of HGF/c-MET signaling results in aberrant β-cell adaptation.[27][28]
c-MET is a receptor tyrosine kinase (RTK) that is activated by its ligand, hepatocyte growth factor (HGF), and is involved in the activation of several cellular processes. When HGF binds c-MET, the receptor homodimerizes and self-phosphorylates to form an SH2 recognition domain. The downstream pathways activated include common signaling molecules such as RAS and MAPK, which affect cell motility, and cell cycle progression.[29]
Studies have shown that HGF is an important signaling molecule in stress related situations where more insulin is needed. Pregnancy causes increased insulin resistance and so a higher insulin demand. The β-cells must compensate for this by either increasing insulin production or proliferating. If neither of the processes occur, then markers for gestational diabetes are observed. It has been observed that pregnancy increases HGF levels, showing a correlation that suggests a connection between the signaling pathway and increased insulin needs. In fact, when no signaling is present, gestational diabetes is more likely to occur.[27]
The exact mechanism of HGF/c-MET regulated β-cell adaptation is not yet known but there are several hypotheses about how the signaling molecules contribute to insulin levels during pregnancy. c-MET may interact with FoxM1, a molecule important in the cell cycle, as FOXM1 levels decrease when c-MET is not present. Additionally, c-MET may interact with p27 as the protein levels increase with c-MET is not present. Another hypothesis says that c-MET may control β-cell apoptosis because a lack of c-MET causes increases cell death but the signaling mechanisms have not been elucidated.[28]
Although the mechanism of HGF/c-MET control of gestational diabetes is not yet well understood, there is a strong correlation between the signaling pathway and the inability to produce an adequate amount of insulin during pregnancy and thus it may be the target for future diabetic therapies.[27][28]
Because glucose travels across the placenta (through diffusion facilitated by GLUT1 carrier), which is located in the syncytiotrophoblast on both the microvillus and basal membranes, these membranes may be the rate-limiting step in placental glucose transport. There is a two- to three-fold increase in the expression of syncytiotrophoblast glucose transporters with advancing gestation. Finally, the role of GLUT3/GLUT4 transport remains speculative. If the untreated gestational diabetes fetus is exposed to consistently higher glucose levels, this leads to increased fetal levels of insulin (insulin itself cannot cross the placenta). The growth-stimulating effects of insulin can lead to excessive growth and a large body (macrosomia). After birth, the high glucose environment disappears, leaving these newborns with ongoing high insulin production and susceptibility to low blood glucose levels (hypoglycemia).[30]
Screening
Non-challenge blood glucose test
|
| Screening glucose challenge test |
| Oral glucose tolerance test (OGTT) |
A number of screening and diagnostic tests have been used to look for high levels of glucose in plasma or serum in defined circumstances. One method is a stepwise approach where a suspicious result on a screening test is followed by diagnostic test. Alternatively, a more involved diagnostic test can be used directly at the first prenatal visit for a woman with a high-risk pregnancy. (for example in those with polycystic ovarian syndrome or acanthosis nigricans).[30]
Non-challenge blood glucose tests involve measuring glucose levels in blood samples without challenging the subject with glucose solutions. A blood glucose level is determined when fasting, two hours after a meal, or simply at any random time. In contrast, challenge tests involve drinking a glucose solution and measuring glucose concentration thereafter in the blood; in diabetes, they tend to remain high. The glucose solution has a very sweet taste which some women find unpleasant; sometimes, therefore, artificial flavours are added. Some women may experience nausea during the test, and more so with higher glucose levels.[31][32]
There is currently not enough research to show which way is best at diagnosing gestational diabetes.[33] Routine screening of women with a glucose challenge test may find more women with gestational diabetes than only screening women with risk factors.[34] Hemoglobin A1c (HbA1c) is not recommended for diagnosing gestational diabetes, as it's a less reliable marker of glycemia during pregnancy than oral glucose tolerance testing (OGTT).[35]
Pathways
Opinions differ about optimal screening and diagnostic measures, in part due to differences in population risks, cost-effectiveness considerations, and lack of an evidence base to support large national screening programs.[36] The most elaborate regimen entails a random blood glucose test during a booking visit, a screening glucose challenge test around 24–28 weeks' gestation, followed by an OGTT if the tests are outside normal limits. If there is a high suspicion, a woman may be tested earlier.[5]
In the United States, most obstetricians prefer universal screening with a screening glucose challenge test.[37] In the United Kingdom, obstetric units often rely on risk factors and a random blood glucose test.[30][38] The American Diabetes Association and the Society of Obstetricians and Gynaecologists of Canada recommend routine screening unless the woman is low risk (this means the woman must be younger than 25 years and have a body mass index less than 27, with no personal, ethnic or family risk factors)[5][36] The Canadian Diabetes Association and the American College of Obstetricians and Gynecologists recommend universal screening.[39][40] The U.S. Preventive Services Task Force found there is insufficient evidence to recommend for or against routine screening,[41] and a 2017 a Cochrane review found that there is not evidence to determine which screening method is best for women and their babies.[34]
Some pregnant women and careproviders choose to forgo routine screening due to the absence of risk factors, however this is not advised due to the large proportion of women who develop gestational diabetes despite having no risk factors present and the dangers to the mother and baby if gestational diabetes remains untreated.[20]
Non-challenge blood glucose tests
When a plasma glucose level is found to be higher than 126 mg/dL (7.0 mmol/L) after fasting, or over 200 mg/dL (11.1 mmol/L) on any occasion, and if this is confirmed on a subsequent day, the diagnosis of GDM is made, and no further testing is required.[5] These tests are typically performed at the first antenatal visit. They are simple to administer and inexpensive, but have a lower test performance compared to the other tests, with moderate sensitivity, low specificity and high false positive rates.[42][43][44]
Screening glucose challenge test
The screening glucose challenge test (sometimes called the O'Sullivan test) is performed between 24 and 28 weeks, and can be seen as a simplified version of the oral glucose tolerance test (OGTT). No previous fasting is required for this screening test,[45] in contrast to the OGTT. The O'Sullivan test involves drinking a solution containing 50 grams of glucose, and measuring blood levels one hour later.[46]
If the cut-off point is set at 140 mg/dL (7.8 mmol/L), 80% of women with GDM will be detected.[5] If this threshold for further testing is lowered to 130 mg/dL, 90% of GDM cases will be detected, but there will also be more women who will be subjected to a consequent OGTT unnecessarily.
Oral glucose tolerance test
A standardized oral glucose tolerance test (OGTT)[47] should be done in the morning after an overnight fast of between 8 and 14 hours. During the three previous days the subject must have an unrestricted diet (containing at least 150 g carbohydrate per day) and unlimited physical activity. The subject should remain seated during the test and should not smoke throughout the test.
IADPSG (International Association of Diabetes and Pregnancy Study Groups) has developed diagnostic criteria for GDM, based on the results of adverse pregnancy outcomes in the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study.[48] These were recommended by WHO 2013.[49]
According to these gestational diabetes mellitus should be diagnosed at any time in pregnancy if one of the following criteria are met, using a 75 g glucose OGTT:
- Fasting blood glucose level ≥92 mg/dL (5.1 mmol/L)
- 1 hour blood glucose level ≥180 mg/dL (10 mmol/L)
- 2 hour blood glucose level ≥153 mg/dL (8.5 mmol/L)
Urinary glucose testing
Women with GDM may have high glucose levels in their urine (glucosuria). Although dipstick testing is widely practiced, it performs poorly, and discontinuing routine dipstick testing has not been shown to cause underdiagnosis where universal screening is performed.[50] Increased glomerular filtration rates during pregnancy contribute to some 50% of women having glucose in their urine on dipstick tests at some point during their pregnancy. The sensitivity of glucosuria for GDM in the first two trimesters is only around 10% and the positive predictive value is around 20%.[51][52]
Prevention
Vitamin D supplementation during pregnancy may help to prevent gestational diabetes.[53] A 2015 review found that when done during pregnancy moderate physical exercise is effective for the prevention of gestational diabetes.[54] A 2014 review however did not find a significant effect.[55] It is uncertain if additional dietary advice interventions help to reduce the risk of gestational diabetes.[56] However, data from the Nurses' Health Study shows that adherence to a healthy plant-based diet is associated with lower risk for GDM.[57] Diet and physical activity interventions designed to prevent excessive gestational weight gain reduce the rates of gestational diabetes. However, the impact of these interventions varies with the body-mass index of the person as well as with the region in which the studies were performed.[58]
Moderate-quality evidence suggest that there is a reduced risk of gestational diabetes mellitus and caesarean section with combined diet and exercise interventions during pregnancy as well as reductions in gestational weight gain, compared with standard care.[59]
A 2023 review found that a plant-based diet (including fruits, vegetables, whole grains, nuts and seeds, and tea) rich in phytochemicals lowers the risk of GDM.[60] A Cochrane review, updated 2023, stated that myo‐inositol has a potential beneficial effect of improving insulin sensitivity, which suggested that it may be useful for women in preventing gestational diabetes″.[61]
It has been suggested that for women who have had gestational diabetes, diet, exercise, education, and lifestyle changes between pregnancies may lower their chances of having gestational diabetes again in future pregnancies.[62] However, there is no research to show whether interventions between pregnancies lower the number of women who develop gestational diabetes again.[62]
Management
Treatment of GDM with diet and insulin reduces health problems mother and child.[63] Treatment of GDM is also accompanied by more inductions of labour.[63]
A repeat OGTT should be carried out 6 weeks after delivery, to confirm the diabetes has disappeared. Afterwards, regular screening for type 2 diabetes is advised.[12]
Lifestyle interventions include exercise, diet advice, behavioural interventions, relaxation, self-monitoring glucose, and combined interventions.[64] Women with gestational diabetes who receive lifestyle interventions seem to have less postpartum depression, and were more likely to reach their weight loss targets after giving birth, than women who had no intervention.[64] Their babies are also less likely to be large for their gestational age, and have less percentage of fat when they are born.[64] More research is needed to find out which lifestyle interventions are best.[64] Some women with GDM use probiotics but it is very uncertain if there are any benefits in terms of blood glucose levels, high blood pressure disorders or induction of labour.[65]
If a diabetic diet or G.I. Diet, exercise, and oral medication are inadequate to control glucose levels, insulin therapy may become necessary.
The development of macrosomia can be evaluated during pregnancy by using sonography. Women who use insulin, with a history of stillbirth, or with hypertension are managed like women with overt diabetes.[20]
Lifestyle
Counselling before pregnancy (for example, about preventive folic acid supplements) and multidisciplinary management are important for good pregnancy outcomes.[66] Most women can manage their GDM with dietary changes and exercise. Self monitoring of blood glucose levels can guide therapy. Some women will need antidiabetic drugs, most commonly insulin therapy.
Any diet needs to provide sufficient calories for pregnancy, typically 2,000–2,500 kcal with the exclusion of simple carbohydrates.[20] The main goal of dietary modifications is to avoid peaks in blood sugar levels. This can be done by spreading carbohydrate intake over meals and snacks throughout the day, and using slow-release carbohydrate sources—known as the G.I. Diet. Since insulin resistance is highest in mornings, breakfast carbohydrates need to be restricted more.[12]
The Mediterranean diet may be associated with reduced incidence of gestational diabetes.[67] However, there is not enough evidence to indicate if one type of dietary advice is better than another.[68]
Regular moderately intense physical exercise is advised, although there is no consensus on the specific structure of exercise programs for GDM.[12][69] Pregnant women who exercise have lower blood sugar levels when fasting and after meals compared to those who do not exercise.[70] It is not clear which form of exercise is best when pregnant.[70]
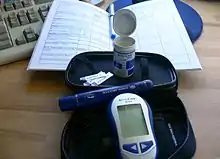
Self monitoring can be accomplished using a handheld capillary glucose dosage system. Compliance with these glucometer systems can be low.[71] There is not a lot of research into what target blood sugar levels should be for women with gestational diabetes and targets recommended to women vary around the world.[72] Target ranges advised by the Australasian Diabetes in Pregnancy Society are as follows:[12]
- fasting capillary blood glucose levels <5.5 mmol/L
- 1 hour postprandial capillary blood glucose levels <8.0 mmol/L
- 2 hour postprandial blood glucose levels <6.7 mmol/L
Regular blood samples can be used to determine HbA1c levels, which give an idea of glucose control over a longer time period.[12]
Research suggests a possible benefit of breastfeeding to reduce the risk of diabetes and related risks for both mother and child.[73]
Medication
If monitoring reveals failing control of glucose levels with these measures, or if there is evidence of complications like excessive fetal growth, treatment with insulin might be necessary. This is most commonly fast-acting insulin given just before eating to blunt glucose rises after meals.[12] Care needs to be taken to avoid low blood sugar levels due to excessive insulin. Insulin therapy can be normal or very tight; more injections can result in better control but requires more effort, and there is no consensus that it has large benefits.[30][74] A 2016 Cochrane review (updated in 2023) concluded that quality evidence is not yet available to determine the best blood sugar range for improving health for pregnant women with GDM and their babies.[72]
There is some evidence that certain medications by mouth might be safe in pregnancy, or at least, are less dangerous to the developing fetus than poorly controlled diabetes. When comparing which diabetes tablets (medication by mouth) work best and are safest, there is not enough quality research to support one medication over another.[75] The medication metformin is better than glyburide.[76] If blood glucose cannot be adequately controlled with a single agent, the combination of metformin and insulin may be better than insulin alone.[76] Another review found good short term safety for both the mother and baby with metformin but unclear long term safety.[77]
People may prefer metformin by mouth to insulin injections.[3] Treatment of polycystic ovarian syndrome with metformin during pregnancy has been noted to decrease GDM levels.[78]
Almost half of the women did not reach sufficient control with metformin alone and needed supplemental therapy with insulin; compared to those treated with insulin alone, they required less insulin, and they gained less weight.[79] With no long-term studies into children of women treated with the drug, there remains a possibility of long-term complications from metformin therapy.[3] Babies born to women treated with metformin have been found to develop less visceral fat, making them less prone to insulin resistance in later life.[79]
Prognosis
Gestational diabetes generally resolves once the baby is born. Based on different studies, the chances of developing GDM in a second pregnancy, if a woman had GDM in her first pregnancy, are between 30 and 84%, depending on ethnic background. A second pregnancy within one year of the previous pregnancy has a large likelihood of GDM recurrence.[80]
Women diagnosed with gestational diabetes have an increased risk of developing diabetes mellitus in the future. The risk is highest in women who needed insulin treatment, had antibodies associated with diabetes (such as antibodies against glutamate decarboxylase, islet cell antibodies and/or insulinoma antigen-2), women with more than two previous pregnancies, and women who were obese (in order of importance).[81][82] Women requiring insulin to manage gestational diabetes have a 50% risk of developing diabetes within the next five years.[83] Depending on the population studied, the diagnostic criteria and the length of follow-up, the risk can vary enormously.[84] The risk appears to be highest in the first 5 years, reaching a plateau thereafter.[84] One of the longest studies followed a group of women from Boston, Massachusetts; half of them developed diabetes after 6 years, and more than 70% had diabetes after 28 years.[84] In a retrospective study in Navajo women, the risk of diabetes after GDM was estimated to be 50 to 70% after 11 years.[85] Another study found a risk of diabetes after GDM of more than 25% after 15 years.[86] In populations with a low risk for type 2 diabetes, in lean subjects and in women with auto-antibodies, there is a higher rate of women developing type 1 diabetes (LADA).[82]
Children of women with GDM have an increased risk for childhood and adult obesity and an increased risk of glucose intolerance and type 2 diabetes later in life.[87] This risk relates to increased maternal glucose values.[88] It is currently unclear how much genetic susceptibility and environmental factors contribute to this risk, and whether treatment of GDM can influence this outcome.[89]
Relative benefits and harms of different oral anti-diabetic medications are not yet well understood as of 2017.[75]
There are scarce statistical data on the risk of other conditions in women with GDM; in the Jerusalem Perinatal study, 410 out of 37,962 women were reported to have GDM, and there was a tendency towards more breast and pancreatic cancer, but more research is needed to confirm this finding.[90][91]
Research is being conducted to develop a web-based clinical decision support system for GDM prediction using machine learning techniques. Results so far demonstrated great potential in clinical practicality for automatic GDM prognosis.[92]
Complications
GDM poses a risk to mother and child. This risk is largely related to uncontrolled blood glucose levels and its consequences. The risk increases with higher blood glucose levels.[93] Treatment resulting in better control of these levels can reduce some of the risks of GDM considerably.[71]
The two main risks GDM imposes on the baby are growth abnormalities and chemical imbalances after birth, which may require admission to a neonatal intensive care unit. Infants born to mothers with GDM are at risk of being both large for gestational age (macrosomic)[93] in unmanaged GDM, and small for gestational age and Intrauterine growth retardation[94] in managed GDM. Macrosomia in turn increases the risk of instrumental deliveries (e.g. forceps, ventouse and caesarean section) or problems during vaginal delivery (such as shoulder dystocia). Macrosomia may affect 12% of normal women compared to 20% of women with GDM.[30] However, the evidence for each of these complications is not equally strong; in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study for example, there was an increased risk for babies to be large but not small for gestational age in women with uncontrolled GDM.[93] In a recent birth cohot study of 5150 deliveries, a research group active at the University of Helsinki and Helsinki University Hospital, Finland demonstrated that the mother's GDM is an independent factor that increases the risk of fetal hypoxia, during labour. The study was published in the Acta Diabetologica in June 2021.[95] Another finding was that GDM increased the susceptibility of the fetus to intrapartum hypoxia, regardless of the size of the fetus.[95] The risk of hypoxia and the resulting risk of poor condition in newborn infants was nearly 7-fold in the fetuses of mothers with GDM compared to the fetuses of non-diabetic mothers.[95] Furthermore, according to the findings, the risk of needing to perform resuscitation on the newborn after birth was 10-fold.[95]
Another finding was that gestational diabetes increased the susceptibility of the fetus to intrapartal hypoxia, regardless of the size of the fetus.
"The risk of hypoxia and the resulting risk of poor condition in newborn infants was nearly seven-fold in the fetuses of mothers with gestational diabetes compared to the fetuses of non-diabetic mothers," says researcher Mikko Tarvonen. According to the findings, the risk of needing to perform resuscitation on the newborn was ten-fold.Research into complications for GDM is difficult because of the many confounding factors (such as obesity). Labelling a woman as having GDM may in itself increase the risk of having an unnecessary caesarean section.[96][97]
Neonates born from women with consistently high blood sugar levels are also at an increased risk of low blood glucose (hypoglycemia), jaundice, high red blood cell mass (polycythemia) and low blood calcium (hypocalcemia) and magnesium (hypomagnesemia).[98] Untreated GDM also interferes with maturation, causing dysmature babies prone to respiratory distress syndrome due to incomplete lung maturation and impaired surfactant synthesis.[98]
Unlike pre-gestational diabetes, gestational diabetes has not been clearly shown to be an independent risk factor for birth defects. Birth defects usually originate sometime during the first trimester (before the 13th week) of pregnancy, whereas GDM gradually develops and is least pronounced during the first and early second trimester. Studies have shown that the offspring of women with GDM are at a higher risk for congenital malformations.[99][100][101] A large case-control study found that gestational diabetes was linked with a limited group of birth defects, and that this association was generally limited to women with a higher body mass index (≥ 25 kg/m2).[102] It is difficult to make sure that this is not partially due to the inclusion of women with pre-existent type 2 diabetes who were not diagnosed before pregnancy.
Because of conflicting studies, it is unclear at the moment whether women with GDM have a higher risk of preeclampsia.[103] In the HAPO study, the risk of preeclampsia was between 13% and 37% higher, although not all possible confounding factors were corrected.[93]
Epidemiology
Gestational diabetes affects 3–10% of pregnancies, depending on the population studied.[3][104]
References
- ↑ "Diabetes Blue Circle Symbol". International Diabetes Federation. 17 March 2006. Archived from the original on 5 August 2007.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 "Gestational Diabetes". NIDDK. September 2014. Archived from the original on 16 August 2016. Retrieved 31 July 2016.
- 1 2 3 4 5 6 7 8 9 10 11 Donovan PJ, McIntyre HD (October 2010). "Drugs for gestational diabetes". Australian Prescriber. 33 (5): 141–144. doi:10.18773/austprescr.2010.066.
- ↑ Metzger BE, Coustan DR (August 1998). "Summary and recommendations of the Fourth International Workshop-Conference on Gestational Diabetes Mellitus. The Organizing Committee". Diabetes Care. 21 (Suppl 2): B161-7. PMID 9704245. And the rest of the issue B1–B167.
- 1 2 3 4 5 American Diabetes Association (January 2004). "Gestational diabetes mellitus". Diabetes Care. 27 Suppl 1 (Supplement 1): S88-90. doi:10.2337/diacare.27.2007.s88. PMID 14693936.
- ↑ White P (November 1949). "Pregnancy complicating diabetes". The American Journal of Medicine. 7 (5): 609–16. doi:10.1016/0002-9343(49)90382-4. PMID 15396063.
- ↑ "Priscilla White - White Classification, Diabetes in Pregnancy". Archived from the original on 2017-03-02. Retrieved 2017-02-20.
- ↑ Gabbe SG, Niebyl JR, Simpson JL (2002). OBSTETRICS: Normal and Problem Pregnancies (Fourth ed.). New York: Churchill Livingstone. ISBN 978-0-443-06572-9.
- 1 2 American Diabetes Association (January 2017). "2. Classification and Diagnosis of Diabetes". Diabetes Care. 40 (Suppl 1): S11–S24. doi:10.2337/dc17-S005. PMID 27979889.
- ↑ Carpenter MW, Coustan DR (December 1982). "Criteria for screening tests for gestational diabetes". American Journal of Obstetrics and Gynecology. 144 (7): 768–73. doi:10.1016/0002-9378(82)90349-0. PMID 7148898.
- ↑ Committee on Practice Bulletins—Obstetrics (February 2018). "ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus". Obstetrics and Gynecology. 131 (2): e49–e64. doi:10.1097/AOG.0000000000002501. PMID 29370047. S2CID 3395229.
- 1 2 3 4 5 6 7 Ross G (June 2006). "Gestational diabetes". Australian Family Physician. 35 (6): 392–6. PMID 16751853.
- ↑ Toulis KA, Goulis DG, Kolibianakis EM, Venetis CA, Tarlatzis BC, Papadimas I (August 2009). "Risk of gestational diabetes mellitus in women with polycystic ovary syndrome: a systematic review and a meta-analysis". Fertility and Sterility. 92 (2): 667–77. doi:10.1016/j.fertnstert.2008.06.045. PMID 18710713.
- ↑ Khandwala YS, Baker VL, Shaw GM, Stevenson DK, Lu Y, Eisenberg ML (October 2018). "Association of paternal age with perinatal outcomes between 2007 and 2016 in the United States: population based cohort study". BMJ. 363: k4372. doi:10.1136/bmj.k4372. PMC 6207919. PMID 30381468.
- ↑ Chu SY, Callaghan WM, Kim SY, Schmid CH, Lau J, England LJ, Dietz PM (August 2007). "Maternal obesity and risk of gestational diabetes mellitus". Diabetes Care. 30 (8): 2070–6. doi:10.2337/dc06-2559a. PMID 17416786.
- ↑ Zhang C, Bao W, Rong Y, Yang H, Bowers K, Yeung E, Kiely M (2013). "Genetic variants and the risk of gestational diabetes mellitus: a systematic review". Human Reproduction Update. 19 (4): 376–90. doi:10.1093/humupd/dmt013. PMC 3682671. PMID 23690305.
- ↑ Yahaya TO, Salisu T, Abdulrahman YB, Umar AK (2020-03-23). "Update on the genetic and epigenetic etiology of gestational diabetes mellitus: a review". Egyptian Journal of Medical Human Genetics. 21 (1): 13. arXiv:2101.07350. doi:10.1186/s43042-020-00054-8. ISSN 2090-2441.
- ↑ Bjørge T, Tretli S, Engeland A (December 2004). "Relation of height and body mass index to renal cell carcinoma in two million Norwegian men and women". American Journal of Epidemiology. 160 (12): 1168–76. doi:10.1093/aje/kwh345. PMID 15583369.
- ↑ Ma RM, Lao TT, Ma CL, Liao SJ, Lu YF, Du MY, Xiao H, Zhang L, Yang MH, Xiao X (November 2007). "Relationship between leg length and gestational diabetes mellitus in Chinese pregnant women". Diabetes Care. 30 (11): 2960–1. doi:10.2337/dc07-0763. PMID 17666468.
- 1 2 3 4 ACOG (December 1994). Precis V. An Update on Obstetrics and Gynecology. ACOG (1994). p. 170. ISBN 978-0-915473-22-9.
- ↑ "Gestational Diabetes". American Pregnancy Association. 27 April 2020. Retrieved 14 October 2020.
- 1 2 Carr DB, Gabbe S (1998). "Gestational Diabetes: Detection, Management, and Implications". Clin Diabetes. 16 (1): 4. Archived from the original on 2007-10-10.
- ↑ Xu J, Zhao YH, Chen YP, Yuan XL, Wang J, Zhu H, Lu CM (2014). "Maternal circulating concentrations of tumor necrosis factor-alpha, leptin, and adiponectin in gestational diabetes mellitus: a systematic review and meta-analysis". TheScientificWorldJournal. 2014: 926932. doi:10.1155/2014/926932. PMC 4151523. PMID 25202741.
- ↑ Gabbe SG (2012). Obstetrics normal and problem pregnancies (6th ed.). Philadelphia: Elsevier/Saunders. p. 890. ISBN 978-1-4557-3395-8.
- ↑ Buchanan TA, Xiang AH (March 2005). "Gestational diabetes mellitus". The Journal of Clinical Investigation. 115 (3): 485–91. doi:10.1172/JCI24531. PMC 1052018. PMID 15765129.
- ↑ Sorenson RL, Brelje TC (June 1997). "Adaptation of islets of Langerhans to pregnancy: beta-cell growth, enhanced insulin secretion and the role of lactogenic hormones". Hormone and Metabolic Research. 29 (6): 301–7. doi:10.1055/s-2007-979040. PMID 9230352. S2CID 46710474.
- 1 2 3 Alvarez-Perez JC, Ernst S, Demirci C, Casinelli GP, Mellado-Gil JM, Rausell-Palamos F, Vasavada RC, Garcia-Ocaña A (January 2014). "Hepatocyte growth factor/c-Met signaling is required for β-cell regeneration". Diabetes. 63 (1): 216–23. doi:10.2337/db13-0333. PMC 3868042. PMID 24089510.
- 1 2 3 Demirci C, Ernst S, Alvarez-Perez JC, Rosa T, Valle S, Shridhar V, Casinelli GP, Alonso LC, Vasavada RC, García-Ocana A (May 2012). "Loss of HGF/c-Met signaling in pancreatic β-cells leads to incomplete maternal β-cell adaptation and gestational diabetes mellitus". Diabetes. 61 (5): 1143–52. doi:10.2337/db11-1154. PMC 3331762. PMID 22427375.
- ↑ Organ SL, Tsao MS (November 2011). "An overview of the c-MET signaling pathway". Therapeutic Advances in Medical Oncology. 3 (1 Suppl): S7–S19. doi:10.1177/1758834011422556. PMC 3225017. PMID 22128289.
- 1 2 3 4 5 Kelly L, Evans L, Messenger D (May 2005). "Controversies around gestational diabetes. Practical information for family doctors". Canadian Family Physician. 51 (5): 688–95. PMC 1472928. PMID 15934273.
- ↑ Sievenpiper JL, Jenkins DJ, Josse RG, Vuksan V (February 2001). "Dilution of the 75-g oral glucose tolerance test improves overall tolerability but not reproducibility in subjects with different body compositions". Diabetes Research and Clinical Practice. 51 (2): 87–95. doi:10.1016/S0168-8227(00)00209-6. PMID 11165688.
- ↑ Reece EA, Holford T, Tuck S, Bargar M, O'Connor T, Hobbins JC (January 1987). "Screening for gestational diabetes: one-hour carbohydrate tolerance test performed by a virtually tasteless polymer of glucose". American Journal of Obstetrics and Gynecology. 156 (1): 132–4. doi:10.1016/0002-9378(87)90223-7. PMID 3799747.
- ↑ Farrar D, Duley L, Dowswell T, Lawlor DA (August 2017). "Different strategies for diagnosing gestational diabetes to improve maternal and infant health". The Cochrane Database of Systematic Reviews. 2017 (8): CD007122. doi:10.1002/14651858.CD007122.pub4. PMC 6483546. PMID 28832911.
- 1 2 Tieu J, McPhee AJ, Crowther CA, Middleton P, Shepherd E (August 2017). "Screening for gestational diabetes mellitus based on different risk profiles and settings for improving maternal and infant health". The Cochrane Database of Systematic Reviews. 2017 (8): CD007222. doi:10.1002/14651858.CD007222.pub4. PMC 6483271. PMID 28771289.
- ↑ Powe CE, Edelson PK (2020-05-27). "HbA1c Can Underestimate Maternal Glycemia During Pregnancy". Massachusetts General Hospital.
- 1 2 Berger H, Crane J, Farine D, Armson A, De La Ronde S, Keenan-Lindsay L, Leduc L, Reid G, Van Aerde J (November 2002). "Screening for gestational diabetes mellitus". Journal of Obstetrics and Gynaecology Canada. 24 (11): 894–912. doi:10.1016/s1701-2163(16)31047-7. PMID 12417905.
- ↑ Gabbe SG, Gregory RP, Power ML, Williams SB, Schulkin J (June 2004). "Management of diabetes mellitus by obstetrician-gynecologists". Obstetrics and Gynecology. 103 (6): 1229–34. doi:10.1097/01.AOG.0000128045.50439.89. PMID 15172857. S2CID 28960551.
- ↑ Mires GJ, Williams FL, Harper V (February 1999). "Screening practices for gestational diabetes mellitus in UK obstetric units". Diabetic Medicine. 16 (2): 138–41. doi:10.1046/j.1464-5491.1999.00011.x. PMID 10229307. S2CID 32186114.
- ↑ Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2003 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2003; 27 (Suppl 2): 1–140.
- ↑ Gabbe SG, Graves CR (October 2003). "Management of diabetes mellitus complicating pregnancy". Obstetrics and Gynecology. 102 (4): 857–68. doi:10.1016/j.obstetgynecol.2003.07.001. PMID 14551019.
- ↑ Hillier TA, Vesco KK, Pedula KL, Beil TL, Whitlock EP, Pettitt DJ (May 2008). "Screening for gestational diabetes mellitus: a systematic review for the U.S. Preventive Services Task Force". Annals of Internal Medicine. 148 (10): 766–75. doi:10.7326/0003-4819-148-10-200805200-00009. PMID 18490689.
- ↑ Agarwal MM, Dhatt GS (February 2007). "Fasting plasma glucose as a screening test for gestational diabetes mellitus". Archives of Gynecology and Obstetrics. 275 (2): 81–7. doi:10.1007/s00404-006-0245-9. PMID 16967273. S2CID 32300456.
- ↑ Sacks DA, Chen W, Wolde-Tsadik G, Buchanan TA (June 2003). "Fasting plasma glucose test at the first prenatal visit as a screen for gestational diabetes". Obstetrics and Gynecology. 101 (6): 1197–203. doi:10.1016/s0029-7844(03)00049-8. PMID 12798525. S2CID 12056832.
- ↑ Agarwal MM, Dhatt GS, Punnose J, Zayed R (April 2007). "Gestational diabetes: fasting and postprandial glucose as first prenatal screening tests in a high-risk population". The Journal of Reproductive Medicine. 52 (4): 299–305. PMID 17506370.
- ↑ GLUCOSE TOLERANCE TEST Archived 2012-12-12 at archive.today at the Dwight D. Eisenhower Army Medical Center. Last Modified November 25, 2009
- ↑ Metzger BE, Biastre SA, Gardner B (2006). "What I need to know about Gestational Diabetes". National Diabetes Information Clearinghouse. Archived from the original on 2006-11-26. Retrieved 2006-11-27.
- ↑ "Glucose screening tests during pregnancy". Medline Plus. U.S. National Library of Medicine. Retrieved 8 November 2018.
- ↑ Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, et al. (May 2008). "Hyperglycemia and adverse pregnancy outcomes". The New England Journal of Medicine. 358 (19): 1991–2002. doi:10.1056/NEJMoa0707943. PMID 18463375.
- ↑ World Health Organization (2013). "Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy". hdl:10665/85975.
- ↑ Rhode MA, Shapiro H, Jones OW (March 2007). "Indicated vs. routine prenatal urine chemical reagent strip testing". The Journal of Reproductive Medicine. 52 (3): 214–9. PMID 17465289.
- ↑ Alto WA (November 2005). "No need for glycosuria/proteinuria screen in pregnant women". The Journal of Family Practice. 54 (11): 978–83. PMID 16266604.
- ↑ Ritterath C, Siegmund T, Rad NT, Stein U, Buhling KJ (2006). "Accuracy and influence of ascorbic acid on glucose-test with urine dip sticks in prenatal care". Journal of Perinatal Medicine. 34 (4): 285–8. doi:10.1515/JPM.2006.054. PMID 16856816. S2CID 7177148.
- ↑ Palacios C, Trak-Fellermeier MA, Martinez RX, Lopez-Perez L, Lips P, Salisi JA, et al. (October 2019). "Regimens of vitamin D supplementation for women during pregnancy". The Cochrane Database of Systematic Reviews. 2019 (10): CD013446. doi:10.1002/14651858.CD013446. PMC 6776191. PMID 31581312.
- ↑ Sanabria-Martínez G, García-Hermoso A, Poyatos-León R, Álvarez-Bueno C, Sánchez-López M, Martínez-Vizcaíno V (August 2015). "Effectiveness of physical activity interventions on preventing gestational diabetes mellitus and excessive maternal weight gain: a meta-analysis". BJOG. 122 (9): 1167–74. doi:10.1111/1471-0528.13429. PMID 26036300. S2CID 36297578.
- ↑ Yin YN, Li XL, Tao TJ, Luo BR, Liao SJ (February 2014). "Physical activity during pregnancy and the risk of gestational diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials". British Journal of Sports Medicine. 48 (4): 290–5. doi:10.1136/bjsports-2013-092596. PMID 24037671. S2CID 13168801.
- ↑ Tieu J, Shepherd E, Middleton P, Crowther CA (January 2017). "Dietary advice interventions in pregnancy for preventing gestational diabetes mellitus". The Cochrane Database of Systematic Reviews. 1 (1): CD006674. doi:10.1002/14651858.CD006674.pub3. PMC 6464792. PMID 28046205.
- ↑ Chen Z, Qian F, Liu G, Li M, Voortman T, Tobias DK, et al. (December 2021). "Prepregnancy plant-based diets and the risk of gestational diabetes mellitus: a prospective cohort study of 14,926 women". The American Journal of Clinical Nutrition. 114 (6): 1997–2005. doi:10.1093/ajcn/nqab275. PMC 8634573. PMID 34510175.
- ↑ Bennett CJ, Walker RE, Blumfield ML, Gwini SM, Ma J, Wang F, et al. (July 2018). "Interventions designed to reduce excessive gestational weight gain can reduce the incidence of gestational diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials". Diabetes Research and Clinical Practice (Review). 141: 69–79. doi:10.1016/j.diabres.2018.04.010. PMID 29698713. S2CID 13660089.
- ↑ Shepherd E, Gomersall JC, Tieu J, Han S, Crowther CA, Middleton P (November 2017). "Combined diet and exercise interventions for preventing gestational diabetes mellitus". The Cochrane Database of Systematic Reviews. 2017 (11): CD010443. doi:10.1002/14651858.cd010443.pub3. PMC 6485974. PMID 29129039.
- ↑ Jaworsky K, DeVillez P, Basu A (February 2023). "The Role of Phytochemicals and Plant-Based Diets in Gestational Diabetes: Evidence from Clinical Trials". International Journal of Environmental Research and Public Health. 20 (5): 4188. doi:10.3390/ijerph20054188. PMC 10001985. PMID 36901197.
- ↑ Soana K Motuhifonuaa, Luling Lina. Jane Alsweiler, Tineke J Crawford, Caroline A Crowther (15 February 2023). "Antenatal dietary supplementation with myo-inositol for preventing gestational diabetes". Cochrane Review. 2023 (2): CD011507. doi:10.1002/14651858.CD011507.pub3. PMC 9930614. PMID 36790138.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - 1 2 Tieu J, Shepherd E, Middleton P, Crowther CA (August 2017). "Interconception care for women with a history of gestational diabetes for improving maternal and infant outcomes". The Cochrane Database of Systematic Reviews. 2017 (8): CD010211. doi:10.1002/14651858.CD010211.pub3. PMC 6483533. PMID 28836274.
- 1 2 Alwan N, Tuffnell DJ, West J (July 2009). "Treatments for gestational diabetes". The Cochrane Database of Systematic Reviews. 2009 (3): CD003395. doi:10.1002/14651858.CD003395.pub2. PMC 7154381. PMID 19588341.
- 1 2 3 4 Brown J, Alwan NA, West J, Brown S, McKinlay CJ, Farrar D, Crowther CA (May 2017). "Lifestyle interventions for the treatment of women with gestational diabetes" (PDF). The Cochrane Database of Systematic Reviews. 2017 (5): CD011970. doi:10.1002/14651858.CD011970.pub2. hdl:10292/10707. PMC 6481373. PMID 28472859.
- ↑ Okesene-Gafa KA, Moore AE, Jordan V, McCowan L, Crowther CA (June 2020). "Probiotic treatment for women with gestational diabetes to improve maternal and infant health and well-being". The Cochrane Database of Systematic Reviews. 2020 (6): CD012970. doi:10.1002/14651858.CD012970.pub2. PMC 7386668. PMID 32575163.
- ↑ Kapoor N, Sankaran S, Hyer S, Shehata H (December 2007). "Diabetes in pregnancy: a review of current evidence". Current Opinion in Obstetrics & Gynecology. 19 (6): 586–90. doi:10.1097/GCO.0b013e3282f20aad. PMID 18007138. S2CID 19468297.
- ↑ Zhang Y, Xia M, Weng S, Wang C, Yuan P, Tang S (December 2022). "Effect of Mediterranean diet for pregnant women: a meta-analysis of randomized controlled trials". The Journal of Maternal-Fetal & Neonatal Medicine. 35 (24): 4824–4829. doi:10.1080/14767058.2020.1868429. PMID 33632052. S2CID 232058447.
- ↑ Han S, Middleton P, Shepherd E, Van Ryswyk E, Crowther CA (February 2017). "Different types of dietary advice for women with gestational diabetes mellitus". The Cochrane Database of Systematic Reviews. 2 (2): CD009275. doi:10.1002/14651858.CD009275.pub3. PMC 6464700. PMID 28236296.
- ↑ Mottola MF (December 2007). "The role of exercise in the prevention and treatment of gestational diabetes mellitus". Current Sports Medicine Reports. 6 (6): 381–6. doi:10.1097/01.csmr.0000305617.87993.51. PMID 18001611. S2CID 220572575.
- 1 2 Brown J, Ceysens G, Boulvain M (June 2017). "Exercise for pregnant women with gestational diabetes for improving maternal and fetal outcomes". The Cochrane Database of Systematic Reviews. 2017 (6): CD012202. doi:10.1002/14651858.CD012202.pub2. PMC 6481507. PMID 28639706.
- 1 2 Langer O, Rodriguez DA, Xenakis EM, McFarland MB, Berkus MD, Arrendondo F (April 1994). "Intensified versus conventional management of gestational diabetes". American Journal of Obstetrics and Gynecology. 170 (4): 1036–46, discussion 1046–7. doi:10.1016/S0002-9378(94)70097-4. PMID 8166187.
- 1 2 Hofer OJ, Martis R, Alsweiler J, Crowther CA (October 2023). "Different intensities of glycaemic control for women with gestational diabetes mellitus". The Cochrane Database of Systematic Reviews. 2023 (10): CD011624. doi:10.1002/14651858.CD011624.pub3. PMC 10563388. PMID 37815094.
- ↑ Taylor JS, Kacmar JE, Nothnagle M, Lawrence RA (October 2005). "A systematic review of the literature associating breastfeeding with type 2 diabetes and gestational diabetes". Journal of the American College of Nutrition. 24 (5): 320–6. doi:10.1080/07315724.2005.10719480. PMID 16192255. S2CID 24794632.
- ↑ Nachum Z, Ben-Shlomo I, Weiner E, Shalev E (November 1999). "Twice daily versus four times daily insulin dose regimens for diabetes in pregnancy: randomised controlled trial". BMJ. 319 (7219): 1223–7. doi:10.1136/bmj.319.7219.1223. PMC 28269. PMID 10550081.
- 1 2 Brown J, Martis R, Hughes B, Rowan J, Crowther CA (January 2017). "Oral anti-diabetic pharmacological therapies for the treatment of women with gestational diabetes". review. The Cochrane Database of Systematic Reviews. 1 (1): CD011967. doi:10.1002/14651858.CD011967.pub2. PMC 6464763. PMID 28120427.
- 1 2 Balsells M, García-Patterson A, Solà I, Roqué M, Gich I, Corcoy R (January 2015). "Glibenclamide, metformin, and insulin for the treatment of gestational diabetes: a systematic review and meta-analysis". BMJ. 350: h102. doi:10.1136/bmj.h102. PMC 4301599. PMID 25609400.
- ↑ Butalia S, Gutierrez L, Lodha A, Aitken E, Zakariasen A, Donovan L (January 2017). "Short- and long-term outcomes of metformin compared with insulin alone in pregnancy: a systematic review and meta-analysis". Diabetic Medicine. 34 (1): 27–36. doi:10.1111/dme.13150. PMID 27150509. S2CID 3418227.
- ↑ Simmons D, Walters BN, Rowan JA, McIntyre HD (May 2004). "Metformin therapy and diabetes in pregnancy". The Medical Journal of Australia. 180 (9): 462–4. doi:10.5694/j.1326-5377.2004.tb06024.x. PMID 15115425. S2CID 43358857.
- 1 2 Sivalingam VN, Myers J, Nicholas S, Balen AH, Crosbie EJ (2014). "Metformin in reproductive health, pregnancy and gynaecological cancer: established and emerging indications". Human Reproduction Update. 20 (6): 853–68. doi:10.1093/humupd/dmu037. PMID 25013215.
- ↑ Kim C, Berger DK, Chamany S (May 2007). "Recurrence of gestational diabetes mellitus: a systematic review". Diabetes Care. 30 (5): 1314–9. doi:10.2337/dc06-2517. PMID 17290037.
- ↑ Löbner K, Knopff A, Baumgarten A, Mollenhauer U, Marienfeld S, Garrido-Franco M, Bonifacio E, Ziegler AG (March 2006). "Predictors of postpartum diabetes in women with gestational diabetes mellitus". Diabetes. 55 (3): 792–7. doi:10.2337/diabetes.55.03.06.db05-0746. PMID 16505245.
- 1 2 Järvelä IY, Juutinen J, Koskela P, Hartikainen AL, Kulmala P, Knip M, Tapanainen JS (March 2006). "Gestational diabetes identifies women at risk for permanent type 1 and type 2 diabetes in fertile age: predictive role of autoantibodies". Diabetes Care. 29 (3): 607–12. doi:10.2337/diacare.29.03.06.dc05-1118. PMID 16505514.
- ↑ Janzen C, Greenspoon JS (2006). "Gestational Diabetes". Diabetes Mellitus & Pregnancy – Gestational Diabetes. Armenian Medical Network. Archived from the original on 2007-01-05. Retrieved 2006-11-27.
- 1 2 3 Kim C, Newton KM, Knopp RH (October 2002). "Gestational diabetes and the incidence of type 2 diabetes: a systematic review". Diabetes Care. 25 (10): 1862–8. doi:10.2337/diacare.25.10.1862. PMID 12351492.
- ↑ Lee AJ, Hiscock RJ, Wein P, Walker SP, Permezel M (April 2007). "Gestational diabetes mellitus: clinical predictors and long-term risk of developing type 2 diabetes: a retrospective cohort study using survival analysis". Diabetes Care. 30 (4): 878–83. doi:10.2337/dc06-1816. PMID 17392549.
- ↑ Boney CM, Verma A, Tucker R, Vohr BR (March 2005). "Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus". Pediatrics. 115 (3): e290-6. doi:10.1542/peds.2004-1808. PMID 15741354.
- ↑ Hillier TA, Pedula KL, Schmidt MM, Mullen JA, Charles MA, Pettitt DJ (September 2007). "Childhood obesity and metabolic imprinting: the ongoing effects of maternal hyperglycemia". Diabetes Care. 30 (9): 2287–92. doi:10.2337/dc06-2361. PMID 17519427.
- ↑ Metzger BE (December 2007). "Long-term outcomes in mothers diagnosed with gestational diabetes mellitus and their offspring". Clinical Obstetrics and Gynecology. 50 (4): 972–9. doi:10.1097/GRF.0b013e31815a61d6. PMID 17982340.
- ↑ Perrin MC, Terry MB, Kleinhaus K, Deutsch L, Yanetz R, Tiram E, Calderon-Margalit R, Friedlander Y, Paltiel O, Harlap S (March 2008). "Gestational diabetes and the risk of breast cancer among women in the Jerusalem Perinatal Study". Breast Cancer Research and Treatment. 108 (1): 129–35. doi:10.1007/s10549-007-9585-9. PMID 17476589. S2CID 2373773.
- ↑ Perrin MC, Terry MB, Kleinhaus K, Deutsch L, Yanetz R, Tiram E, Calderon R, Friedlander Y, Paltiel O, Harlap S (August 2007). "Gestational diabetes as a risk factor for pancreatic cancer: a prospective cohort study". BMC Medicine. 5 (1): 25. doi:10.1186/1741-7015-5-25. PMC 2042496. PMID 17705823.
- ↑ Du Y, Rafferty AR, McAuliffe FM, Wei L, Mooney C (January 2022). "An explainable machine learning-based clinical decision support system for prediction of gestational diabetes mellitus". Scientific Reports. 12 (1): 1170. Bibcode:2022NatSR..12.1170D. doi:10.1038/s41598-022-05112-2. PMC 8782851. PMID 35064173.
- 1 2 3 4 Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, McIntyre HD, Oats JJ, Persson B, Rogers MS, Sacks DA (May 2008). "Hyperglycemia and adverse pregnancy outcomes" (PDF). The New England Journal of Medicine. 358 (19): 1991–2002. doi:10.1056/NEJMoa0707943. PMID 18463375.
- ↑ Setji TL, Brown AJ, Feinglos MN (1 January 2005). "Gestational Diabetes Mellitus". Clinical Diabetes. 23 (1): 17–24. doi:10.2337/diaclin.23.1.17.
- 1 2 3 4 Tarvonen M, Hovi P, Sainio S, Vuorela P, Andersson S, Teramo K (2021). "Intrapartal cardiotocographic patterns and hypoxia-related perinatal outcomes in pregnancies complicated by gestational diabetes mellitus". Acta Diabetologica. 58 (11): 1563–1573. doi:10.1007/s00592-021-01756-0. PMC 8505288. PMID 34151398.
- ↑ Naylor CD, Sermer M, Chen E, Farine D (November 1997). "Selective screening for gestational diabetes mellitus. Toronto Trihospital Gestational Diabetes Project Investigators". The New England Journal of Medicine. 337 (22): 1591–6. doi:10.1056/NEJM199711273372204. PMID 9371855.
- ↑ Jovanovic-Peterson L, Bevier W, Peterson CM (April 1997). "The Santa Barbara County Health Care Services program: birth weight change concomitant with screening for and treatment of glucose-intolerance of pregnancy: a potential cost-effective intervention?". American Journal of Perinatology. 14 (4): 221–8. doi:10.1055/s-2007-994131. PMID 9259932. S2CID 23520352.
- 1 2 Jones CW (September 2001). "Gestational diabetes and its impact on the neonate". Neonatal Network. 20 (6): 17–23. doi:10.1891/0730-0832.20.6.17. PMID 12144115. S2CID 34954951.
- ↑ Allen VM, Armson BA (November 2007). "Teratogenicity associated with pre-existing and gestational diabetes". Journal of Obstetrics and Gynaecology Canada. 29 (11): 927–934. doi:10.1016/s1701-2163(16)32653-6. PMID 17977497.
- ↑ Martínez-Frías ML, Frías JP, Bermejo E, Rodríguez-Pinilla E, Prieto L, Frías JL (June 2005). "Pre-gestational maternal body mass index predicts an increased risk of congenital malformations in infants of mothers with gestational diabetes". Diabetic Medicine. 22 (6): 775–81. doi:10.1111/j.1464-5491.2005.01492.x. PMID 15910631. S2CID 13356040.
- ↑ Savona-Ventura C, Gatt M (August 2004). "Embryonal risks in gestational diabetes mellitus". Early Human Development. 79 (1): 59–63. doi:10.1016/j.earlhumdev.2004.04.007. PMID 15449398.
- ↑ Correa A, Gilboa SM, Besser LM, Botto LD, Moore CA, Hobbs CA, Cleves MA, Riehle-Colarusso TJ, Waller DK, Reece EA (September 2008). "Diabetes mellitus and birth defects". American Journal of Obstetrics and Gynecology. 199 (3): 237.e1–9. doi:10.1016/j.ajog.2008.06.028. PMC 4916956. PMID 18674752.
- ↑ Leguizamón GF, Zeff NP, Fernández A (August 2006). "Hypertension and the pregnancy complicated by diabetes". Current Diabetes Reports. 6 (4): 297–304. doi:10.1007/s11892-006-0064-1. PMID 16879782. S2CID 2430661.
- ↑ Schneider C. "Diabetes and the Risk to Your Family Tree". www.diabetescare.net. Diabetescare.net. Archived from the original on 10 December 2014. Retrieved 5 December 2014.
External links
- IDF Diabetes Atlas
- International Diabetes Federation
- National Institute of Child Health and Human Development – Am I at Risk for Gestational Diabetes?
- National Institute of Child Health and Human Development – Managing Gestational Diabetes: A Patient's Guide to a Healthy Pregnancy
- Gestational Diabetes Resource Guide – American Diabetes Association
- Diabetes.co.uk: Gestational Diabetes
| |||||||||||||||||
| Sexual health |
| ||||||||||||||||
| Non-reproductive health |
| ||||||||||||||||
| Sociocultural factors | |||||||||||||||||
| Politics, Research & Advocacy |
| ||||||||||||||||
| Women's health by country | |||||||||||||||||
| |||||||||||||||||
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||
| |||||||||||||||||