| Bankart lesion | |
|---|---|
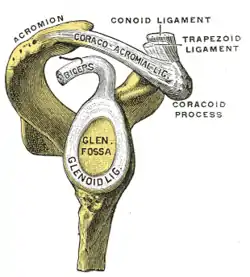 | |
| The glenoid labrum, labeled glenoid ligament, is damaged in a Bankart lesion. Lateral view demonstrating the articular surface of the right scapula is shown. | |
| Symptoms | Shoulder instability and widespread shoulder discomfort, and catching, locking, or popping feelings in shoulders.[1] |
| Risk factors | Anterior shoulder dislocation and/or repeated anterior shoulder subluxations.[2] |
| Diagnostic method | X-ray and MRI. |
| Differential diagnosis | Anterior labroligamentous periosteal sleeve avulsion, Rotator Cuff Tears, SLAP Lesion, Impingement, Perthes lesion, Glenolabral articular disruption, Humeral avulsion of the glenohumeral ligament.[2] |
A Bankart lesion is a type of shoulder injury that occurs following a dislocated shoulder.[3] It is an injury of the anterior (inferior) glenoid labrum of the shoulder.[4] When this happens, a pocket at the front of the glenoid forms that allows the humeral head to dislocate into it. It is an indication for surgery and often accompanied by a Hill-Sachs lesion, damage to the posterior humeral head.[5]
A bony Bankart is a Bankart lesion that includes a fracture of the anterior-inferior glenoid cavity of the scapula bone.[6]
The Bankart lesion is named after English orthopedic surgeon Arthur Sydney Blundell Bankart (1879–1951).[7]
Signs and symptoms
Bankart lesions are characterized by recurrent shoulder instability and widespread shoulder discomfort. Some individuals may experience catching, locking, or popping feelings in their shoulders. The majority of Bankart lesion patients have primary or recurrent anterior shoulder dislocation.[1]
Diagnosis
The diagnosis is usually initially made by a combination of physical exam and medical imaging, where the latter may be projectional radiography (in cases of bony Bankart) and/or MRI of the shoulder. The presence of intra-articular contrast allows for better evaluation of the glenoid labrum.[8] Type V SLAP tears extends into the Bankart defect.[9]
Treatment
Arthroscopic repair of Bankart injuries have good success rates, though nearly one-third of patients require further surgery for continued instability after the initial procedure in a study of young adults, with higher re-operation rates in those less than 20 years of age.[10] Options for repair include an arthroscopic technique or a more invasive open Latarjet procedure,[11] with the open technique tending to have a lower incidence of recurrent dislocation, but also a reduced range of motion following surgery.[12]
Gallery
 X-ray at left shows anterior dislocation in a young man after trying to get up from his bed. X-ray at right shows same shoulder after reduction and internal rotation, revealing both a bony Bankart lesion and a Hill-Sachs lesion.
X-ray at left shows anterior dislocation in a young man after trying to get up from his bed. X-ray at right shows same shoulder after reduction and internal rotation, revealing both a bony Bankart lesion and a Hill-Sachs lesion. CT scan showing a bony Bankart lesion at the antero-inferior glenoid
CT scan showing a bony Bankart lesion at the antero-inferior glenoid MRI of the shoulder after an anterior dislocation showing a Hill-Sachs lesion and labral Bankart lesion
MRI of the shoulder after an anterior dislocation showing a Hill-Sachs lesion and labral Bankart lesion
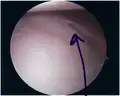 Bankart lesion seen at arthroscopy
Bankart lesion seen at arthroscopy Radiograph showing a bony Bankart lesion with stationary fragment at the inferior glenoid
Radiograph showing a bony Bankart lesion with stationary fragment at the inferior glenoid 3-D CT reconstruction of a bankart lesion which occurred post anterior shoulder dislocation. This subject's humerus remains mildly superiorly subluxated. Fracture marked by a black arrow.
3-D CT reconstruction of a bankart lesion which occurred post anterior shoulder dislocation. This subject's humerus remains mildly superiorly subluxated. Fracture marked by a black arrow.
See also
References
- 1 2 Tupe, Rishikesh N.; Tiwari, Vivek (August 3, 2023). "Anteroinferior Glenoid Labrum Lesion (Bankart Lesion)". StatPearls Publishing. PMID 36508533. Retrieved October 30, 2023.
- 1 2 "Bankart lesion". Physiopedia. Retrieved October 30, 2023.
- ↑ Major, Nancy M.; Anderson, Mark W. (2020). "10. Shoulder". Musculoskeletal MRI. Philadelphia: Elsevier. pp. 218–219. ISBN 978-0-323-415606.
- ↑ Widjaja A, Tran A, Bailey M, Proper S (2006). "Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation". ANZ Journal of Surgery. 76 (6): 436–8. doi:10.1111/j.1445-2197.2006.03760.x. PMID 16768763. S2CID 42257934.
- ↑ Porcellini, Giuseppe; Campi, Fabrizio; Paladini, Paolo (2002). "Arthroscopic approach to acute bony Bankart lesion". Arthroscopy: The Journal of Arthroscopic and Related Surgery. 18 (7): 764–769. doi:10.1053/jars.2002.35266. ISSN 0749-8063. PMID 12209435.
- ↑ "bony Bankart at The Steadman Clinic Vail, CO. © 2001 by LeadingMD". Archived from the original on 2011-07-26. Retrieved 2011-05-16.
- ↑ Who Named It.com - Bankart's Lesion
- ↑ Jana, M; Srivastava, DN; Sharma, R; Gamanagatti, S; Nag, H; Mittal, R; Upadhyay, AD (April 2011). "Spectrum of magnetic resonance imaging findings in clinical glenohumeral instability". The Indian Journal of Radiology & Imaging. 21 (2): 98–106. doi:10.4103/0971-3026.82284. PMC 3137866. PMID 21799591.
- ↑ Chang, D; Mohana-Borges, A; Borso, M; Chung, CB (October 2008). "SLAP lesions: anatomy, clinical presentation, MR imaging diagnosis and characterization". European Journal of Radiology. 68 (1): 72–87. doi:10.1016/j.ejrad.2008.02.026. PMID 18499376.
- ↑ Flinkkilä, T; Knape, R; Sirniö, K; Ohtonen, P; Leppilahti, J (16 March 2017). "Long-term results of arthroscopic Bankart repair: Minimum 10 years of follow-up". Knee Surgery, Sports Traumatology, Arthroscopy. 26 (1): 94–99. doi:10.1007/s00167-017-4504-z. PMID 28303281. S2CID 6692528.
- ↑ Zimmermann, SM; Scheyerer, MJ; Farshad, M; Catanzaro, S; Rahm, S; Gerber, C (7 December 2016). "Long-Term Restoration of Anterior Shoulder Stability: A Retrospective Analysis of Arthroscopic Bankart Repair Versus Open Latarjet Procedure" (PDF). The Journal of Bone and Joint Surgery. American Volume. 98 (23): 1954–1961. doi:10.2106/jbjs.15.01398. PMID 27926676. S2CID 24940288.
- ↑ Wang, L; Liu, Y; Su, X; Liu, S (8 October 2015). "A Meta-Analysis of Arthroscopic versus Open Repair for Treatment of Bankart Lesions in the Shoulder". Medical Science Monitor. 21: 3028–35. doi:10.12659/msm.894346. PMC 4603609. PMID 26446430.
External links
- Bankart lesion - zadeh.co.uk
{kind=link}